
When “Autism Friendly” Isn’t Enough
How the NHS's Own Digital Tools Could Close the Accessibility Gap - If Anyone Used Them

A poster on the wall. A sensory box in the corner. These are not reasonable adjustments. For autistic patients with communication needs, the NHS has a structural problem - and the solution is already written into its own digital infrastructure.
There is a gap between what NHS policy says and what autistic patients experience. Across the country, GP practices display “autism friendly” branding and point to mandatory staff training. Yet autistic patients continue to face systems built entirely around verbal, real-time communication - the precise mode of interaction that many find most difficult, least reliable, and most anxiety-inducing.
This is not a gap of intention. It is a gap of implementation. And it is, in many cases, unlawful.
The structural problem
The primary communication route in most NHS GP practices today is the eConsult platform. Patients submit queries electronically and are then called back - within a broad, unspecified window, such as “between 9am and 12pm” - by a GP on the telephone.
For an autistic patient, this system creates compounding barriers at every stage.
— eConsult’s open-text fields are restricted to roughly 500 characters per section - approximately 75 to 100 words - making it impossible to explain complex or multi-faceted conditions in a single submission. This is particularly apparent in the management of comorbid health conditions and chronic disease.
— Emails are not accepted. Phone contact is restricted to patients without internet access. There is no written alternative.
— Callback windows are unpredictable, preventing preparation. An autistic patient cannot guarantee they will be in a quiet, private environment with written notes to hand when the call arrives. They cannot guarantee they have a notebook to hand to take notes from the callback.
— When the call does come, patients are asked to verbally recall and expand upon information they already provided in writing - despite the character limits that prevented them from providing it fully in the first place.
The system restricts written communication. Then it demands verbal expansion of that restricted content. For autistic patients - particularly those for whom real-time verbal communication significantly increases cognitive load - this is not a neutral inconvenience. It is a structural disadvantage built into the process itself.
“A disabled patient apologising for navigating a structurally inaccessible system. That is what this produces.”
What the law requires
The legal framework is not ambiguous. Under the Equality Act 2010, healthcare providers have a duty to make reasonable adjustments for disabled people to avoid placing them at a substantial disadvantage. This duty is anticipatory - providers must not wait for patients to struggle before acting.
The Accessible Information Standard (NHS England, 2016) requires that communication needs are identified, recorded, and met. The Health and Care Act 2022 reinforces this further. The NHS’s own Reasonable Adjustment Digital Flag (RADF) was specifically designed to make these needs visible across every point of care, from GP to A&E to dental.
These are not optional standards. They are legal obligations. And for many autistic patients, they are not being met.
The Oliver McGowan Training Question
The NHS mandates The Oliver McGowan Mandatory Training on Learning Disability and Autism to reduce healthcare inequalities for autistic patients. Its intention is clear and important.
But when its principles are not embedded into day-to-day clinical practice, it functions as procedural compliance rather than meaningful cultural change. Training that is not followed by adjusted behaviour is not training. It is a box ticked.
If this training is designed to reduce inequality, why does implementation so often depend entirely on the patient repeatedly advocating for themselves?
Posters are not adjustments
Many practices display “autism friendly” signage. Some provide sensory boxes. These things are not inherently wrong - but they are insufficient, and for many autistic patients they can feel actively misleading.
Autism adjustments are not primarily about sensory needs. For a significant number of autistic people, communication is the central issue. Neuro-affirming practice means:
— Reading a Health Passport or Communication Passport before an appointment.
— Acting on reasonable adjustments recorded in the patient’s notes - without being prompted by the patient.
— Providing written summaries of consultations without being asked.
— Avoiding demands for verbal recall of information already provided in writing.
— Offering predictable, specific contact times so patients can prepare.
— Recognising that “autism friendly” is not a brand - it is a daily practice.
A sensory box in the waiting room does not address processing speed. It does not address working memory. It does not address the anxiety of an unpredictable callback window or the cognitive load of a verbal consultation. Sensory accommodation and communication accommodation are not the same thing.
Why training alone will not fix this
The gap between policy and practice in NHS autism care is not, in most cases, a result of malice. It is a result of institutional culture that defaults to verbal, real-time, unstructured communication - and then leaves it to individual clinicians to deviate from that default.
The problem with relying on individual clinician goodwill is that it is inconsistent, unsustainable, and still places the burden on the patient to advocate at every single interaction. It means that a patient with clearly documented reasonable adjustments can receive an appropriate consultation on Monday and an entirely inappropriate one on Friday, depending on which GP picks up the phone.
Cultural change that relies only on training and goodwill will always be partial and fragile. What is needed is a mechanism that encodes adjustments directly into clinical workflow - that forces the question before the clinician even opens their mouth.
That mechanism already exists.
The solution: using the RADF as a lever for systemic change
The NHS Reasonable Adjustment Digital Flag (RADF) on NHS Spine is designed to surface patient-specific needs at every point of care. When correctly populated, it appears on every NHS system a clinician opens - from the GP’s screen to the A&E dashboard - before they speak to or about the patient.
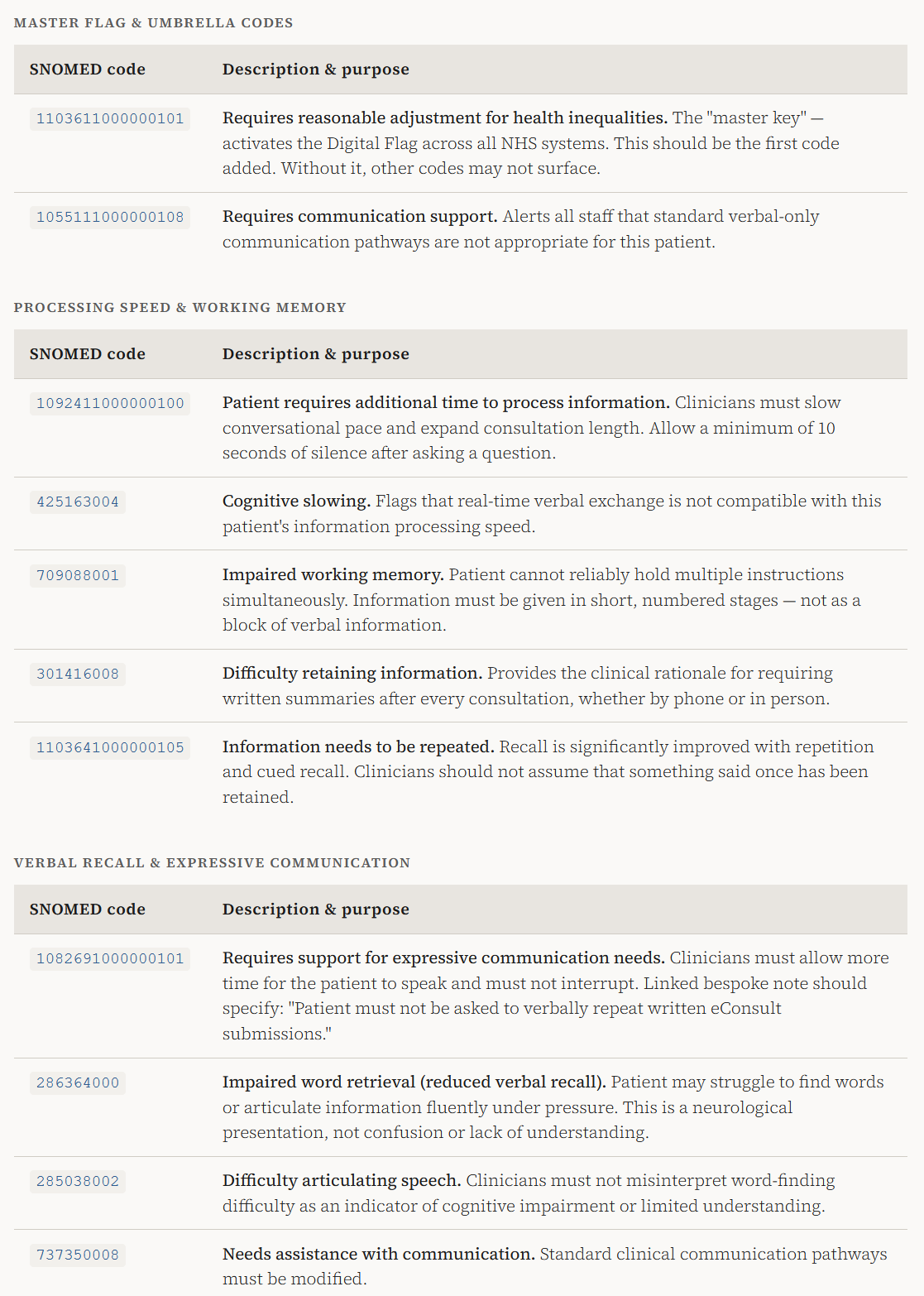
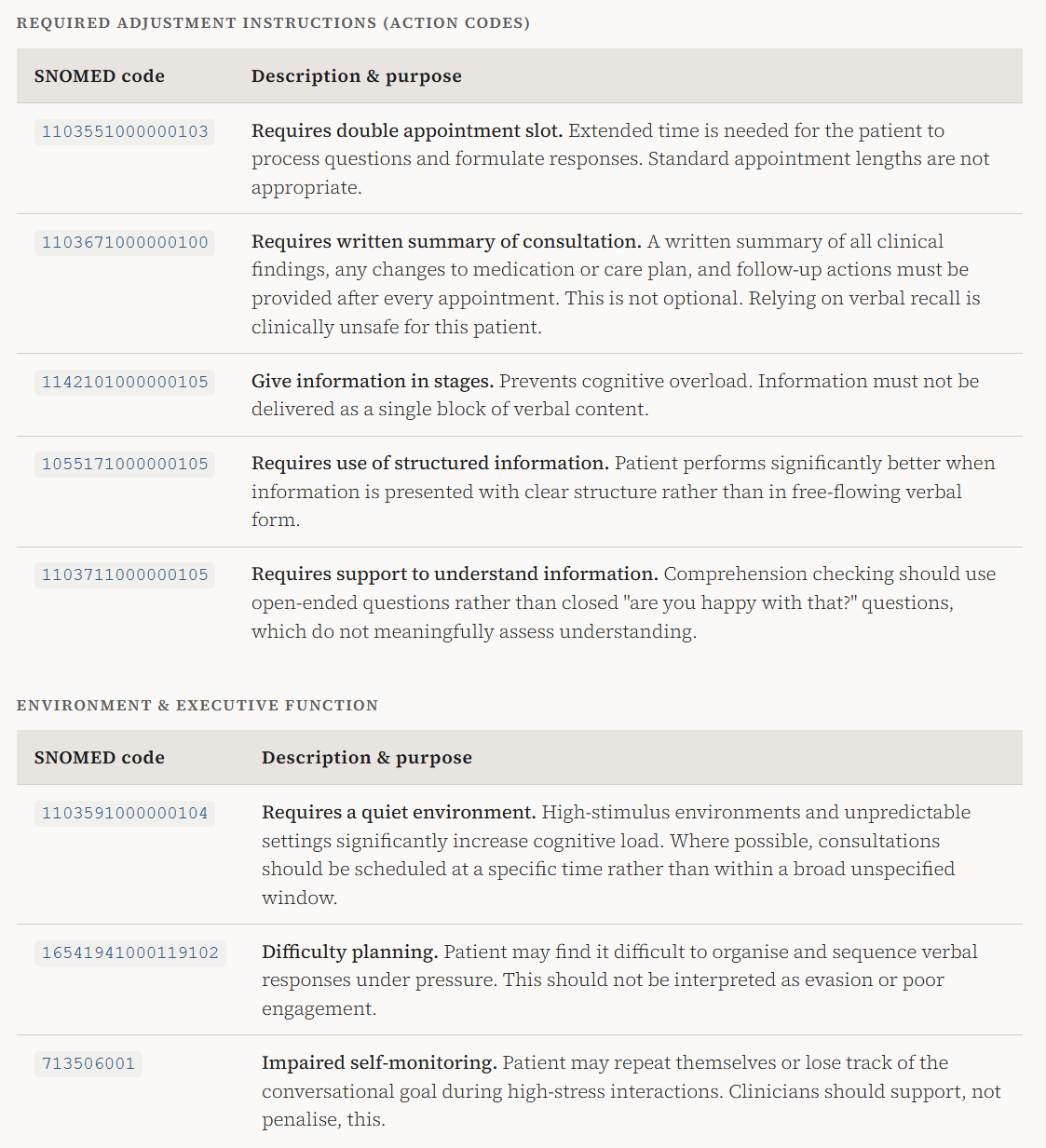
The RADF supports SNOMED CT codes: specific, standardised, machine-readable clinical codes that record not just diagnoses but functional needs and required actions. Used properly, these codes do not simply note that a patient has autism. They instruct the clinician, clearly and specifically, how to adapt their behaviour.
This is the missing link between policy and practice. Not another training module. Not another poster. Specific, actionable codes embedded in the record, surfaced automatically, that tell every clinician exactly what they need to do differently.
A vague entry such as “patient has difficulties retaining information” is a legacy placeholder. It does not instruct. It does not protect. It does not meet NHS Digital Flag standards. It allows clinicians to overlook adjustments without realising they are doing so.
The following tables set out the SNOMED CT codes that autistic patients - particularly those with communication-related needs - should request be added to their Reasonable Adjustment Digital Flag. Autistic patients, advocates, and clinicians working in this space should be aware of them.
The bespoke note: beyond codes
The RADF system also allows for a bespoke free-text note of up to 5,000 characters alongside SNOMED codes. This is where specific, patient-level instructions can be recorded that no standard code fully captures. For example:
Example bespoke RADF note
“This patient communicates more accurately and safely in writing. Patient must not be asked to verbally repeat information already provided in a written eConsult submission. A written summary must be provided after every consultation. Telephone callbacks must be at a specific agreed time, not within a broad unspecified window. Patient has submitted a Health and Communication Passport - this must be read before any consultation. Do not interpret word-finding difficulty as a lack of understanding. The patient’s core intelligence and language comprehension are not affected.”
This is not asking for the extraordinary. It is asking for what has already been promised.
What autistic patients can do
Patients should not have to know all of this. But in the current environment, many do - because the system still places the burden of implementation on those least able to carry it.
If you are autistic and experiencing barriers to appropriate communication in NHS primary care, you have the right to:
— Request that your RADF be reviewed and updated with specific SNOMED CT codes matching your functional needs - not vague legacy placeholder entries.
— Request that a bespoke free-text note be added setting out your specific adjustments in plain language.
— Ask your GP to add the code 1103611000000101 (the master flag) if it is not already active, as without it other adjustments may not surface across the system.
— Provide a Health Passport or Communication Passport and request that a code flagging its existence be added to the RADF so any clinician is immediately directed to it.
— Formally request written communication as a reasonable adjustment under the Equality Act 2010, and follow this with a written record of the request.
— If reasonable adjustments are not followed, raise a formal complaint to the practice and, if unresolved, to the Integrated Care Board - citing the Equality Act 2010, the Accessible Information Standard, and the Health and Care Act 2022.
This post does not constitute legal advice. The SNOMED CT codes listed are drawn from NHS Digital Flag guidance and publicly documented clinical terminology. If you are experiencing difficulty accessing healthcare due to autism or another disability, the Equality Advisory and Support Service (EASS) helpline and your local Patient Advice and Liaison Service (PALS) can provide further support.
